If you’re searching for an hcg levels by week chart, you’re probably trying to understand what a lab result (or home urine test) might mean for early pregnancy, miscarriage follow-up, or an ectopic pregnancy screening context. The most important thing to know upfront: hCG results should be interpreted by a clinician in context of gestational dating, symptoms, and lab-specific reference ranges. Still, you can use a structured framework—test type + timing + trend—to make your results easier to discuss with your healthcare team.
This guide explains hCG hormone levels, the difference between quantitative vs qualitative hCG testing, how to read typical ranges “safely,” and what patterns often prompt repeat testing. You’ll also find targeted sections on beta hCG after miscarriage, hcg level in ectopic pregnancy, and hCG levels in pregnancy with twins, plus a brief note on documentation using an icd-10 code for hcg screening.
What is hCG (human chorionic gonadotropin)?
What hCG is and when it starts to rise in pregnancy
Human chorionic gonadotropin (hCG) is a hormone produced by trophoblast tissue in early pregnancy. As pregnancy progresses, hCG generally rises—especially in the early weeks—before later patterns change. Because the rise depends on how far along you are (and sometimes the exact timing of implantation), two people with similar dates can have different numbers.
Clinicians use hCG in early pregnancy assessment and follow-up because it can reflect whether pregnancy tissue is present and whether hormone levels are changing as expected.
hcg medical term / what the lab reports as (hCG vs beta-hCG)
You may see multiple terms on lab paperwork:
- hCG (general term)
- beta-hCG (commonly reported form in blood tests)
In many clinical settings, “beta-hCG” is the measurable target, and your report will usually include:
- Units (for example, mIU/mL)
- Reference ranges by gestational age (vary by lab)
- Test type (quantitative vs qualitative)
For foundational biology, see: Human Chorionic Gonadotropin (hCG) — StatPearls (NCBI Bookshelf).
Quantitative vs qualitative hCG tests (and when each is used)
This is the “interpretation gap” where many generic charts fall short. A chart may look similar across the internet, but the meaning of a result depends heavily on whether your test is qualitative or quantitative.
Qualitative hCG (poc hcg qualitative) — what “positive/negative” means
Qualitative hCG tests answer a yes/no question: is hCG detected above the test’s threshold? That’s why you might see:
- Negative (below the detection threshold)
- Positive (above the detection threshold)
POC hCG qualitative commonly refers to point-of-care or rapid tests (often urine-based). These tests can be useful for screening, but they typically cannot tell you how close you are to a “range by week” because they don’t provide a numeric value.
Important: “Positive” doesn’t confirm how the pregnancy is developing, and “Negative” doesn’t rule out pregnancy if timing is early.
Quantitative hCG blood test — why numbers matter
A quantitative test gives an actual number (e.g., mIU/mL). This is why quantitative results are often paired with follow-up testing to assess trend—for example, how levels change over 48 hours.
When people search “what are hcg levels in pregnancy,” they’re usually looking for a chart of numeric typical ranges. Those can help you understand the lab’s context, but the safest way to use a chart is:
- Confirm the test type (qualitative vs quantitative)
- Confirm the gestational dating basis used by the lab (LMP vs ultrasound dating)
- Compare the value to your lab’s reference range, not a generic chart alone
- Discuss repeat testing if dates are uncertain or symptoms exist
HCG test midstream vs other urine/blood approaches (high-level)
You may hear about:
- Midstream urine pregnancy tests (often qualitative, home-based)
- Urine quantitative testing (less common)
- Blood quantitative beta-hCG (commonly used for medical evaluation)
Urine tests are convenient, but they’re affected by urine concentration, timing, and detection thresholds. Blood tests are generally preferred when clinicians need to evaluate trends closely.
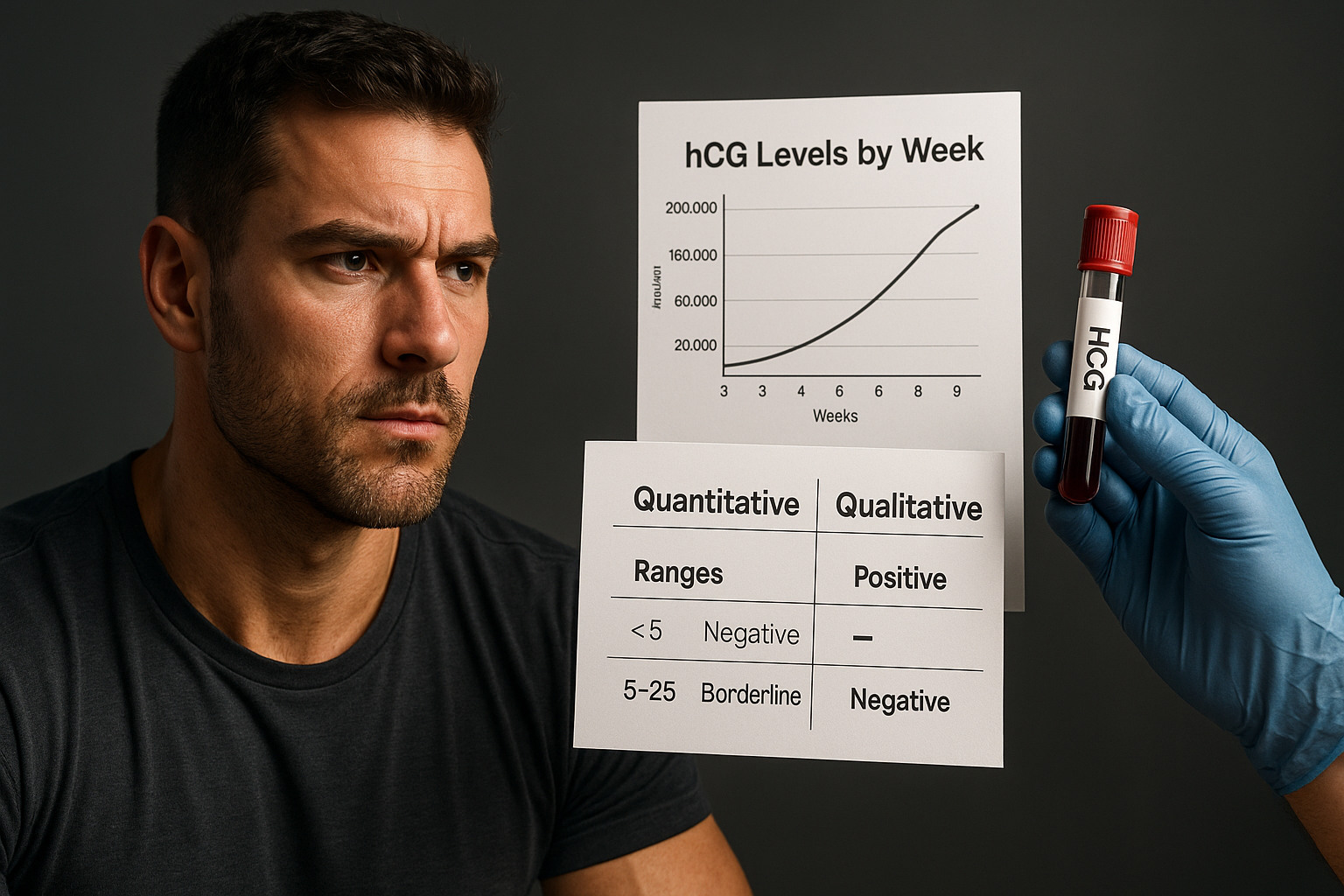
hCG levels by week chart (typical ranges)
The phrase hcg levels by week chart is extremely common, but it’s also easy to misuse. Typical charts show “expected ranges” based on prior clinical observations; however, levels vary widely between individuals and between labs, and gestational dating can be off by a week or more.
Safe use principle: Treat a chart as a conversation starter—not a diagnosis tool.
How to read “hcg levels by week chart” safely (timing varies)
When comparing your result to a chart, consider these factors:
- Dating method: LMP-based estimates vs ultrasound dating
- Test type: qualitative “positive/negative” cannot be compared to numeric ranges
- Lab reference ranges: each lab may have different cutoff values and “by week” categories
- Trend matters: a single value is often less informative than serial testing
- Biologic variability: some healthy pregnancies have lower or higher values than the average
If you want one quick “how to interpret responsibly” checklist, use this with your clinician:
- What test did I have (qualitative vs quantitative, urine vs blood)?
- What units are reported, and what are the lab’s reference ranges for my gestational week?
- Given my timing, do you recommend repeat testing (and when)?
- How will my symptoms factor into the plan?
hcg of 1 — what “near/below detection” can mean (interpretation disclaimer)
Seeing something like “hCG of 1” on a report can be confusing. Depending on the lab’s cutoff, an hCG value near detection may mean:
- Very low or negative-level hCG (below the lab’s positivity threshold)
- Early pregnancy detection before levels rise significantly
- Possible non-pregnancy explanations (which would require clinician assessment)
Bottom line: values near the detection limit are often interpreted using the test’s threshold plus repeat testing and clinical context—not by a chart alone.
Special scenarios: how hCG trends can differ
Searchers often look for a single number in these scenarios. Clinically, however, the safest framework is still test type + timing + trend, with repeat testing when appropriate.
hcg level in ectopic pregnancy (screening context + urgency note)
An hcg level in ectopic pregnancy can vary—some people have relatively low numbers, others have values that overlap with other situations. That’s why clinicians usually rely on a combination of:
- Symptoms (pain, bleeding, dizziness)
- Serial quantitative beta-hCG testing
- Ultrasound findings
Seek urgent care now if you have symptoms that could suggest ectopic pregnancy, such as severe abdominal/pelvic pain, heavy bleeding, dizziness, or fainting. Don’t wait for chart-based interpretation.
hcg levels and miscarriage (beta hCG after miscarriage follow-up concept)
When people ask about hcg levels and miscarriage and beta hCG after miscarriage, they’re often trying to confirm what “normal” decline looks like. Key points:
- A single value can be misleading.
- Clinicians often follow a pattern of falling beta-hCG after pregnancy loss.
- Exact expectations depend on baseline levels, timing, and whether any tissue remains.
If you’re in miscarriage follow-up, the best next step is to ask the clinician or lab ordering provider: what trend are they looking for and when should repeat testing be done? This is safer than trying to match a generic “drop” chart.
hcg levels in pregnancy with twins (general “may be higher” framing)
Many people search what are hcg levels in pregnancy with twins. In general, twin pregnancies may produce higher hCG hormone levels than some singleton pregnancies, but overlap is common. Your plan should still be based on:
- Ultrasound dating and confirmation
- Serial quantitative results when indicated
- Your lab’s reference range interpretation
So instead of expecting “twins = specific number,” think: twins can shift the distribution upward, but charts can’t confirm multiples alone.
How laboratories interpret results (and why units differ)
Two labs can show different numbers at “the same week” because of how they measure hCG (assay method), timing, and reference categories. Always prioritize the report you received.
frer hcg level (clarify as “urine pregnancy test context” if used; explain label ambiguity)
You might encounter terms like “FRER” in discussions of early detection tests. In practice, some products label sensitivity as an “hCG level” cutoff (often based on urine tests). That label can be confusing because:
- Home test sensitivity doesn’t match the exact format of blood quantitative results
- Urine concentration and timing vary
- A “threshold” is not the same as a gestational-age chart value
If your report includes a numeric value, follow the lab’s units and reference ranges. If it’s a home test label, treat it as a detection threshold, not a measurement of pregnancy viability.
“hcg reconstitution calculator” and other calculator terms — when calculators are appropriate vs not
You may see “calculator” language online. For example, “hCG reconstitution calculator” often appears in contexts unrelated to pregnancy blood test interpretation (for medication use or dosing discussions). If you’re asking about medication preparation, dosing safety depends on the specific prescription, concentration, and clinician instructions.
For pregnancy interpretation, the safest “calculator” is usually not an online tool—it’s:
- The lab’s report (units + reference ranges)
- Serial testing dates
- Clinician interpretation in context
If you tell your clinician what tools you’ve found online, they can explain why those tools may or may not apply to your specific test format.
ICD-10 code and screening documentation
Sometimes clinicians and facilities document lab orders using specific diagnostic/procedure codes. If you’re searching for an icd-10 code for hcg screening, the key is that codes can vary based on the clinical reason for testing and local billing practices.
icd-10 code for hcg screening (use as documentation-focused section)
There isn’t one universally correct ICD-10 code that applies to all “hCG screening.” The correct code usually depends on why the test was ordered (for example, suspected pregnancy, evaluation after pregnancy loss, symptoms, follow-up monitoring, etc.).
Practical takeaway: If you need documentation details for an insurance form or medical record request, ask your ordering clinician’s office (or the lab/billing department) which code was used on your specific test order.
When to contact a clinician (action checklist)
Use this checklist to convert a confusing result into clear next steps. It’s also the best way to handle the common problem of uncertain dates.
Ask for repeat testing and trend discussion when dates are uncertain
Contact your clinician or the ordering provider promptly if:
- You had uncertain conception timing or irregular cycles
- You saw a very low/near-threshold value (including “hCG of 1” type reports)
- Your qualitative result was positive but pregnancy dating is unclear
- You have symptoms such as persistent pelvic pain, significant bleeding, dizziness, or fainting
- You’re in follow-up for hcg levels and miscarriage or concerns after pregnancy loss
- Ectopic pregnancy is part of your evaluation (especially with pain/bleeding)
When repeat testing is common: clinicians often recommend serial quantitative beta-hCG testing and sometimes ultrasound, using the combination to interpret progress safely.
FAQ: hCG levels, charts, and test types
What are hcg levels in pregnancy, and how quickly do they rise?
hCG hormone levels typically rise in early pregnancy. The exact pattern varies between individuals and depends on gestational dating and lab method. Because timing can shift by days to weeks, clinicians often focus on trends using quantitative beta-hCG rather than a single value.
What’s the difference between quantitative vs qualitative hCG?
Qualitative tests (often urine) tell you whether hCG is detected above a threshold (“positive/negative”). Quantitative tests (commonly blood) provide a numeric beta-hCG value, which allows trend-based interpretation.
How do hcg levels and miscarriage relate to beta hCG trends after miscarriage?
After pregnancy loss, clinicians typically look for declining beta-hCG over time. A single measurement may not be enough; repeat testing and clinical context matter for safe follow-up.
What is the typical hcg level in ectopic pregnancy, and why is repeat testing important?
There isn’t one “typical” hCG level in ectopic pregnancy because values can overlap with other scenarios. That’s why repeat quantitative beta-hCG testing and ultrasound findings are often used together. If you have severe pain, heavy bleeding, or dizziness/fainting, seek urgent care.
Can hcg levels in pregnancy with twins be higher than singleton pregnancies?
They may be higher, but overlap is common. Twins are confirmed with ultrasound, not by matching hCG numbers to a chart.
What does an hcg of 1 mean on a lab report?
An “hCG of 1” is usually near the detection limit, and the meaning depends on the lab’s assay and positivity cutoff. It often requires clinical context and sometimes repeat quantitative testing rather than chart-based interpretation alone.
Conclusion: what to do next with your hCG results
If your goal is to understand an hcg levels by week chart, the most responsible next step is to map your lab result to the correct framework: quantitative vs qualitative, accurate timing, and trend if repeat testing is indicated. If you’re unsure about your dating or your result is near a detection threshold, ask your clinician what repeat testing schedule they recommend.
Next step: Gather your lab report (units, reference range, and whether it’s quantitative beta-hCG) and discuss it with your clinician—especially if you have symptoms that could indicate ectopic pregnancy.
Related hormone/lab interpretation reading (internal):
- estrogen and weight gain: high vs low estrogen, HRT, and what to do next
- What Is GHRP-2? Benefits, GHRP-2 Side Effects, and GHRP-2 Dosage Per Day
- HGH Peptides: What They Are, Side Effects, Reddit Claims, Cost
Medical disclaimer: This article is for education only and is not a substitute for medical advice, diagnosis, or treatment. hCG results should be interpreted by a clinician in context of gestational dating, symptoms, and lab-specific reference ranges. Charts and typical ranges are examples and vary by lab and measurement method. If you have symptoms suggestive of ectopic pregnancy (such as severe pain, bleeding, dizziness, or fainting), seek urgent care.